 Prof. Joseph Levine, M.D. is an emeritus associate professor in the Division of Psychiatry, Faculty of Health Sciences, Ben Gurion University in Israel. Prof. Levine is a certified psychiatrist with clinical experience in controlled trials of adult psychiatric disorders and in psychotherapy. He was awarded a NRSAD independent investigator grant for the study of Creatine Monohydrate in psychiatric disorders -- mainly Schizophrenia. He resides and treats patients in Tel Aviv and all of central Israel.
Prof. Joseph Levine, M.D. is an emeritus associate professor in the Division of Psychiatry, Faculty of Health Sciences, Ben Gurion University in Israel. Prof. Levine is a certified psychiatrist with clinical experience in controlled trials of adult psychiatric disorders and in psychotherapy. He was awarded a NRSAD independent investigator grant for the study of Creatine Monohydrate in psychiatric disorders -- mainly Schizophrenia. He resides and treats patients in Tel Aviv and all of central Israel.
Conversation 17: Sensitivity Channels and Trigger Event Analysis
Dear readers:
We know that excessive stress can lead to averse changes in our well-being and sometimes even to outburst of a psychiatric disorder. In 1967, psychiatrists Thomas Holmes and Richard Rahe examined over 5000 patient’s medical records to determine whether stressful events cause illnesses. Their premise was that stressors can be ranked by the degree of change or upheaval they typically cause in individuals’ lives. The scale lists common stressful events and arbitrarily assigns a value of 50 ‘LCUs’ [units] to the stress caused by marriage. Patients ranked a list of 43 life events based on a relative score. The Holmes and Rahe Social Readjustment Rating Scale (SRRS) uses the correlational research method to identify the connection between stress and health. Some authors criticized the Holmes and Rahe Stress Scale for not taking into account that different cultural groups react differently to different life events. Also, the scale doesn’t consider intraindividual divergence.
In our own experience we ran into a patient from whom we learned that taking into account interindividual divergence is absolutely crucial in order to predict patient’s reaction to the stressors or, as we mostly name it,”triggers”.
Benny (pseudonym) has worked in a leading position in a City Hall. In his life, he experienced two major traumatic events: one was his 21 year son’s death in a car accident and the other one was his transfer to another position in the City Hall that didn’t cause him any financial losses but was experienced by him as a drop in his social status. After the first event he reacted with a normative grieve reaction. After the second event he got severely depressed and made a serious suicide attempt jumping from the 4th floor that luckily didn’t result in his death.
This patient made us clear that an individual reacts to all possible triggers in a for him/her unique and specific way. This predisposition is likely inborn and is a part of the person’s Primary Self. The same trigger that may have a profound impact upon one particular individual may leave another one totally unaffected. The personal sensitivity to specific triggers is categorized in exactly the same way as the triggers themselves. That means that each person will exhibit sensitivity (or lack of it) to such issues as changes in status, RG [Reference Group] norms, attachments, threats, routine, and energy resources in a for him/her specific way. We call the corresponding personal sensitivities – Sensitivity Channels. For example, if a person is sensitive to changes in his /her status (as our patient we talked about before) and the corresponding changes are imposed on him/her by the social environment, there will be a high probability for averse mental response in case that his status is negatively affected and vice versa there will be a high probability for positive mental response if the status is raised.
This will be true for a person with a high affinity for status changes, but there may be also rare cases where the raise in status affects a person negatively. In such cases the reaction can be expected to be the opposite in comparison with the former description.
One of the important theoretical elaborations in RGFT [Reference Group Focused Therapy] is Trigger Event Analysis (TEA).
TEA is the lifetime analysis of person’s triggers.
TEA divides all triggers leading to some kind of mental breakdown into 6 categories: Status, Norms, Attachment, Threat, Routine, Energy (in a parallel to the existing Sensitivity Channels). These triggers have either explicit or implicit social characteristics, which means that they are associated with patients’ RGs (either internal or external ones). The given context of mental deterioration leads to the conclusion that these triggers have to be regarded as negative triggers – events that precipitate deterioration in mental states.
We can find the position of the Sensitivity Channels (as part of the Primary Self) in the figure below that summarizes our theoretical model of the psyche:
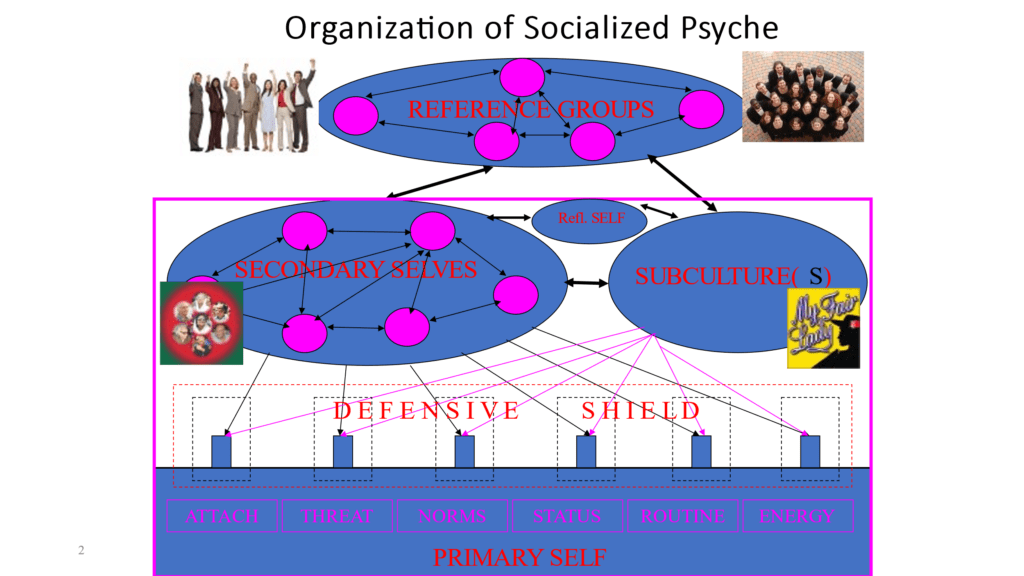
Explanations to the figure:
Primary Self: is a psychical structure that develops prior to socialization. Socialization in the sense of RGFT overlaps greatly with the same term in social psychology and thus does not include the first two years of life prior to language acquisition and prior to the brain ability to internalize integrative aspects of the other object (or him/herself), including perception, cognition, emotion, and behavior.
Secondary Self: is a psychical structure that develops in a process of socialization. It represents the internal image and is a result of internalization of the corresponding RG (that could be a single person or a group of persons). Secondary Self comprises following characteristics (that in a way resemble a blue print of a corresponding person/group): perceptional, cognitional, emotional, and behavioral patterns.
Dictator Self: is a subtype of a Secondary Self which Reflective Self is tightly identified with. It is thus the most dominant among the Secondary Selves and influences greatly a person’s perceptional, emotional, cognitive, and behavioral pattern.
Reflective Self: is a psychical structure that represents a person’s autonomic ability to evaluate a given situation and to choose a corresponding adaptive response.
Subculture: is a source of a social influence upon a person that can not be inferred or deduced from any specific RG effect but is a result of an integrative impact of a certain social environment as a whole.
Defensive Shield: is a variety of mostly unconscious adaptive mechanisms that a person develops in order to diminish a negative impact on his/her Sensitivity Channels.
Trigger Event Analysis (trigger categorization):
Negative trigger is defined as an event that precipitates mental deterioration. It has to stand with this deterioration in both time and causal relation. We categorize such a trigger as belonging to one of the following types:
1. Change in Status within RG
2. Conflict with RG associated Norms
3. Altering (or threat of altering) in a set of important personal Attachments
4. Threat to person’s survival (physical or economical)
5. Rapid change in Daily Routine
6. Changes (Deterioration) in person’s Energetic resources
Change of status within RG
As examples of such a trigger may serve changes in work position, deterioration of marital relations, significant lottery win etc.
Conflict with RG associated norms
Examples: RG pressure on a person to commit an action inconsistent with person’s moral norms, inability to comply with RG norms (because of the intellectual gradient, for example), unwillingness to accept RG norms, consequences of a violation of RG norms (that result in some punitive response on the RG side), etc.
Altering (or threat of altering) in a set of important personal attachments
Death of significant other, breaking relations with a lover, interruption of a physical contact with significant other (drafting to the army, entering a boarding school), on another hand we have such events as child birth, marriage, entering a new RG group (new job, beginning of studies), etc. Altering in a set of personal attachments to a pet or a highly valued object (e.g. collector’s item) is treated in a similar way
Threat to person’s survival (physical or economical)
To this category belong financial problems, severe life-threatening disease, etc.
Rapid change in daily routine
Here can be mentioned such examples as moving to a new location, vacation, change in working routine, role change (becoming a parent, going into pension, drafting to the army for example), etc.
Deterioration of person’s energetic resources
Overworking, sleep deprivation, unbalanced meals or under eating, accompanying disease – may account for examples
Trigger Event Analysis (TEA) helps us to identify the core patient’s problems that have to be addressed.
The triggers are compared against the relevant RGs. If triggers are associated with only a limited number of specific external RGs, then the problem is likely to be with those external groups – RGFT for external groups (RGFT ext.) is advised. If triggers are more or less evenly distributed among different external RGs – probably problem with the patient himself. In this case, RGFT for internalized groups (RGFT int) is advised. The more detailed description of the corresponding treatment interventions will appear in the following blogs.
Yours
Dr Igor Salganick & Prof Joseph Levine
Leave a comment