 Prof. Joseph Levine, M.D. is an emeritus associate professor in the Division of Psychiatry, Faculty of Health Sciences, Ben Gurion University in Israel. Prof. Levine is a certified psychiatrist with clinical experience in controlled trials of adult psychiatric disorders and in psychotherapy. He was awarded a NRSAD independent investigator grant for the study of Creatine Monohydrate in psychiatric disorders -- mainly Schizophrenia. He resides and treats patients in Tel Aviv and all of central Israel.
Prof. Joseph Levine, M.D. is an emeritus associate professor in the Division of Psychiatry, Faculty of Health Sciences, Ben Gurion University in Israel. Prof. Levine is a certified psychiatrist with clinical experience in controlled trials of adult psychiatric disorders and in psychotherapy. He was awarded a NRSAD independent investigator grant for the study of Creatine Monohydrate in psychiatric disorders -- mainly Schizophrenia. He resides and treats patients in Tel Aviv and all of central Israel.
Conversation 73: Understanding paranoid disorder in light of the novel model of the Self
Greetings to our readers,
Paranoid (delusional) disorder is a serious mental condition characterized by persistent delusions – strong beliefs about things that are not based on reality.
Unlike other psychotic disorders such as schizophrenia, people with paranoid disorder often function normally in many aspects of life, except for the influence of their delusions. According to DSM-5-TR (Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, Revised), paranoid disorder is classified as a distinct psychiatric condition that requires specific diagnostic criteria. Understanding the definition, symptoms and treatment options for paranoid disorder is essential for effective management and improving the quality of life of those affected.
How does the DSM-5-TR define paranoid disorder?
Paranoid disorder, as defined by the DSM-5-TR, is a psychotic disorder characterized by the presence of one or more paranoid thoughts lasting at least one month. These paranoid thoughts, which are permanent false beliefs, stand out because they persist despite clear evidence to the contrary.
Unlike other psychotic disorders, people with paranoid disorder usually do not exhibit other prominent psychotic symptoms such as disorganized thinking, hallucinations, or severe dysfunction.
Their behavior outside of the psychotic context often appears normal, allowing them to maintain daily activities and relationships.
The DSM-5-TR establishes specific criteria to differentiate delusions from related conditions such as schizophrenia, in which the delusions are usually accompanied by more severe cognitive and functional impairments. Understanding this disorder requires a clear distinction between the types of false thoughts experienced and how they affect the individual's perception of reality.
What are the main symptoms of paranoid disorder?
In paranoid disorder, the false beliefs are often non-bizarre, meaning they involve situations that could theoretically happen in real life. Examples include a false belief that the person is being followed, that a famous person likes the patient, or that there is a conspiracy against the patient. These false beliefs are plausible but not true.
B) Absence of other psychotic symptoms.
Unlike other psychotic disorders, people with paranoid disorder typically do not experience hallucinations, disorganized speech, or disorganized behavior. If hallucinations occur, they are usually related to the delusional theme and are not prominent.
C) Normal functioning outside of false beliefs.
Outside of their delusions, people with paranoid disorder tend to have relatively normal thinking and functioning. Their daily lives may remain relatively unaffected, unlike schizophrenia, where functioning is more widely impaired.
The DSM-5-TR classifies delusions into specific subtypes, which help clinicians identify the nature of the delusions:
Erotomaniac: Belief that someone, often of a higher status, is in love with a person.
Grandiose: Belief in extraordinary abilities, wealth or fame.
Jealousy: belief that a partner is cheating without proof.
Persecution: Belief that a person is being abused, spied on or conspired against.
Somatic: A belief related to bodily functions or sensations, such as the false belief of being physically ill or infested with parasites.
Duration.
The delusions must last at least 1 month, in order to differentiate paranoid disorder from short-term psychotic episodes or other short-term mental disorders.
Paranoid disorder is a complex condition without a single, well-defined trigger. Instead, a combination of biological, psychological and environmental factors can contribute to its development. Some of the factors or "triggers" that have been linked to paranoid disorder include:
Stressful life events: Intense or prolonged stress, such as the loss of a loved one, divorce, or major life transitions, can sometimes precipitate paranoid thinking.
Social isolation: Lack of strong social support or chronic loneliness may increase risk by limiting reality-checking interactions.
Basic personality factors: People with pre-existing traits such as distrust or suspicion (as seen in paranoid personality traits) may be more vulnerable.
Biological factors: Neurochemical imbalances, genetic predisposition, or structural changes in the brain (including those associated with aging or neurological conditions) may contribute.
Medical conditions or drug use: Certain medical conditions (eg, dementia, Parkinson's disease) or drug use (including side effects from certain drugs) have also been associated with the onset of symptoms of paranoid disorder.
Because paranoid disorder is multifactorial, the specific triggers can vary significantly from person to person, and it is often the interplay of these factors rather than a single factor that leads to the condition.
In our model, the self includes the components of the human psyche mechanism. The model first assumes the existence of the "primary self", which is in fact the basic biological nucleus consisting of a number of innate structures and subject to development during life, this self includes the instinctive emotional and cognitive parts of the person.
The primary self uses the reservoirs and mechanisms of emotion, memory and cognitive abilities and it contains initial nuclei for the future development of other mental structures.
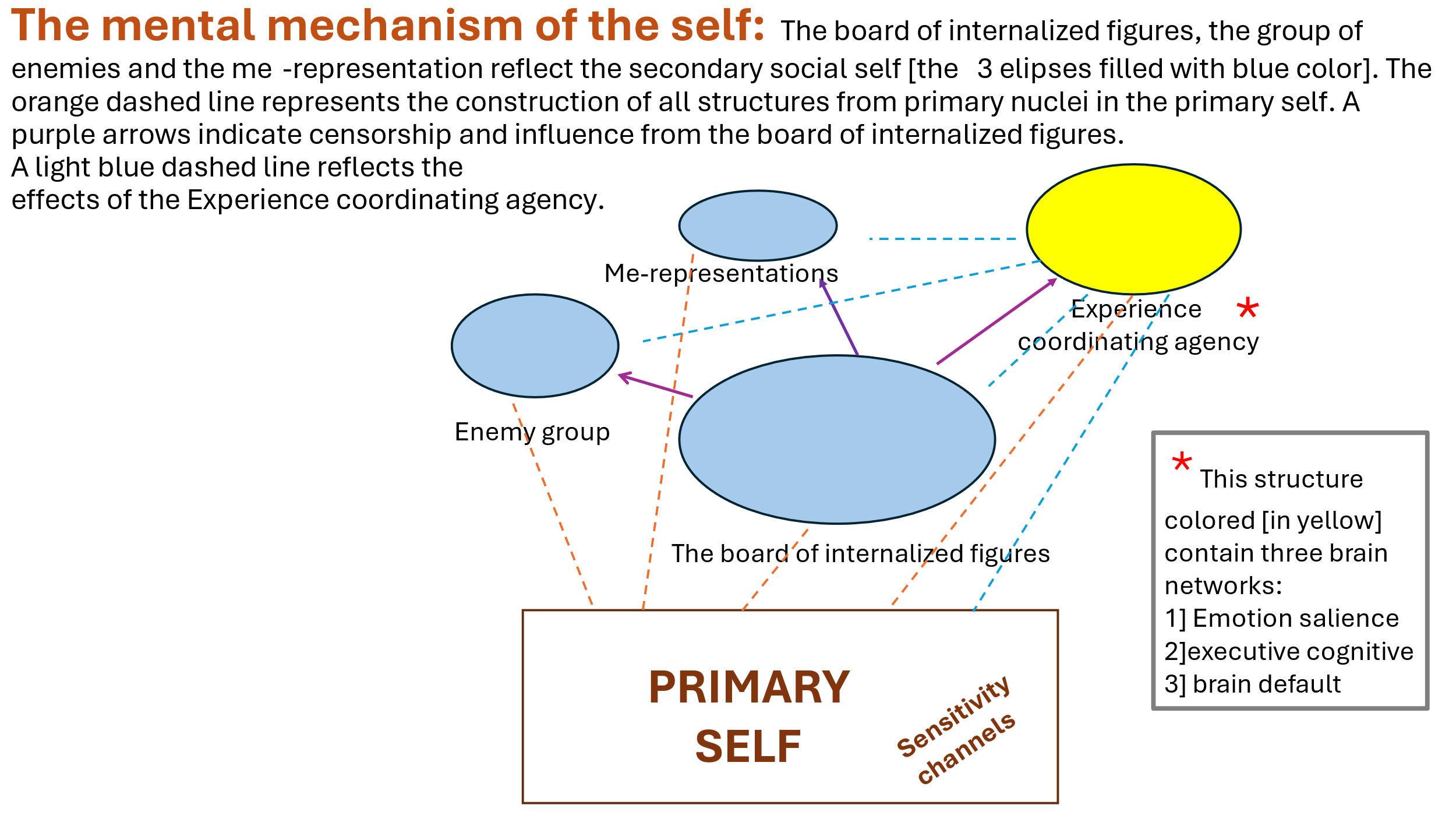
Illustration of our new proposed self-model.
Let us first refer to the primary self (biological predestined core): the primary self consists of innate biological structures and instincts that form the innate basis of the parts of the personality and it also included the cognitive processes and the emotional processes.
This primary self has its own dynamics during a person's life and is subject to changes with age, following diseases, traumas, drug consumption, addiction, etc.
Both the instincts and the basic needs in each and every person change according to different periods of development and aging – hence their effect on behavior) and may change through drugs, trauma, diseases and more.
Within the primary self there is a potential for instrumental abilities that are innate, but they can also be promoted, or on the contrary, suppressed through the influence of the reference groups.
The primary self also has cognitive abilities that are partly innate and partly dependent on interactions with the environment in the first years of life. In addition, it includes the temperament and emotional intelligence that are partly innate and partly dependent on interactions with the environment in the first years of life.
And finally, it includes an energy charge that is mostly innate but can be suppressed through the influence of the reference groups, as well as through various situational factors.
The primary self also includes the seven channels of personal sensitivity: Individual Sensitivity Channels (ISC) that reflect our personal reactivity in response to stressors (both external and internal).
So far we have identified seven channels of sensitivity:
1. Sensitivity regarding one's status and location (status channel)
2. Sensitivity to changes in norms (norms channel)
3. Sensitivity regarding emotional attachment to others (attachment channel)
4. Sensitivity to threat of any kind – physical, economic, etc. (threat channel)
5. Sensitivity to routine changes (routine channel)
6. Sensitivity to a change in energy level and the ability to act derived from it (energy channel)
7. Sensitivity to proprioceptive stimuli coming from the body (proprioceptive channel).
From the primary self, a number of superstructures continue to develop from innate nuclei that form the basis for the development of the baby and later the person throughout his life with the characters around him: three structures that together make up the secondary self or the social self, these include:
A] The group of internalized characters that we will metaphorically call the board or directorate of internalized characters,
B] the group of internalized enemies (enemies’ group),
C] the group of internalized self-representations.
The set of internalized characters consists of internalizations of influential figures in human life, arranged in a hierarchical order [as mentioned, we metaphorically call the group of these internalizations the board of internalized characters or the directorate of internalized characters].
These characters have a continuous dialogue between them and sometimes even conflicts, while one or more of the internalized characters have the greatest influence on the attitudes, feelings and behavior of the individual, which we called the "leader self" [a character formerly also called the "dictator self", see previous talks].
The attitudes of the inner leader play a central role in making decisions about the internalization of information and characters. He decides whether to reject the internalization or, if accepted, in what form it will be internalized. In other words, in a sense, we assume that this influential figure is also a form of internal censorship.
It should be emphasized that these are not concrete hypotheses regarding the presence of internalized figures in the inner world of the individual as a kind of "little people inside the brain", but rather in their representation in different brain areas whose nature and manner of representation still require further research.
We will also note that although we call this figure the "internal leader", with the exception of a certain type, his characteristics are not the same as those of a ruler in a certain country, but rather that this figure is dominant and influential among the "board of characters".
We note that the events and characters in the external world maintain a kind of dialogue mediated by the "experience coordinating agency" [see previous conversations] with the internalized characters on the board [or with the internalized enemies’ group – see below] and may affect the expression and sometimes even the hierarchy of the characters on the internalized characters board.
In addition, it is possible that, similar to short-term memory, parts of which are transferred to long-term memory, also when it comes to the internalization of figures for the board, there is a short-term internalization that, depending on the circumstances, importance and duration of the character's influence, will eventually be transferred to long-term internalization in the board of internalized characters.
Below is the structure of the internalized figures board:
This board consists of "secondary selves" which include the following types:
1) Representations of internalized figures that originate from the significant figures that the person was exposed to during his life, but as mentioned, there may also be imaginary characters represented in books, movies, etc. that greatly influenced the person.
2) internalized representations of "subculture" [subculture refers to social influences in the environment in which a person lives and are not necessarily related to a specific person].
We note that a person is usually unaware that his actions, feelings and attitudes are caused by the dynamic relationships between these structured characters. We will add that internalized key figures in the board of directors [usually human], usually refer to the significant people in a person's life who played central roles in shaping his attitudes, beliefs, values and self-concept.
These figures may include family members, friends, mentors, teachers, or any other influential person who has left a lasting impression on the person's psyche.
Sometimes, these will also include historical, literary and other figures that left a noticeable mark on the person and were internalized by him. The term "internalized" implies that the influence of these key figures has been absorbed and integrated into the individual's thoughts, attitudes, and behaviors.
This internalization occurs through a process of observing, interacting with, and learning from these important people. As a result, the individual may adopt certain values, perspectives, and approaches to life that mirror those of the influential figures. These internalized characters can serve as guiding forces in decision-making, moral thinking and emotional regulation.
Now we will note, in addition, that coming from the primary self there developes a structure that we will call the “enemies’ group”. Thus, in addition to the board of internalized characters, in the social self there is also the "enemies’ group" and more precisely the "group of internalized enemies".
This is the place where the characters that significantly threaten the person are internalized, while the dominant characters in the character board prevent them from entering and internalizing within the characters’
board (we assumed the existence of this group in the last year in light of the thought of the evolutionary need of animals and humans to create such a group for their survival, see a broad reference to the subject of enemies below).
The characters in the "enemies’ group" are characters with a negative emotional value and are represented schematically in relation to the characters in the internalized characters’ board. We note that usually the transition between the board of internalized characters and the group of enemies is not common and even rare and usually happens following the traumatic or threatening event to a person.
In addition, from the primary self, as mentioned, there develops a supergroup of self-representations in the different periods of life [for example, the self-representation as a child, as a teenager, as an adult, etc.], including the representations of the body. The representation of the self in a certain sense is also a kind of container for the information flow of emotional attitudes and behaviors from the dynamics in the characters’ board.
We will note that each of the internalized characters in the board of characters and the internalizations in the group of enemies and the group of ego representations possess their own attitudes.
While the leader figure (or figures) on the internalized board exemplify the most senior and dominant positions in the hierarchy of board figures, they may censor characters who will or will not join the board if their attitudes are contrary to those of the leader or leaders, and will sometimes even join the enemies’ group if they pose a significant threat to the internalized leader or leaders on the board.
In general, the classification of attitudes can be understood as the way in which these internal contents of the individual shape his perceptions, feelings and behaviors in relation to the social world. These positions not only store information, but also determine how incoming stimuli are processed and how responses are generated.
In general, attitudes are divided into three main categories: relational, perceptual and conduct (aor action) attitudes.
Relational attitudes relate to the emotional evaluations people attribute to people, objects, events, or even abstract concepts. These attitudes express how much we love, fear or even loathe something, and form part of the basis of our interpersonal relationships. The strength of these positions is directly related to the significance we attribute to the subject they are related to.
For example, how we feel about close family members versus strangers is mediated by our relational attitudes, which in turn influence our social roles.
Relational attitudes are influenced by many factors, including personal experiences, logical thinking, and social influences that strengthen or challenge our emotional bonds. Attitudes are also related to the functioning of the sensitivity channels—such as those related to status, attachment, and threat—that help determine the emotional valence (positive or negative) and strength of these attitudes.
Perceptual attitudes are more cognitive in nature. They include the mental frameworks or hypotheses that people develop to understand both the physical and the social world. Essentially, these approaches act as lenses through which we interpret and organize our experiences.
Whether derived from personal encounters or acquired from social reference groups, perceptual attitudes guide our assumptions about cause and effect, enabling us to predict and navigate future events.
They contribute to what is sometimes called a "worldview" or "Weltanschauung" – an integrated network of beliefs that filters incoming information. Perceptual attitudes also provide the basis for prediction and decision-making, balancing social truths against individual experiences. The experience coordinating agency is affected by this type of experiences.
Conduct (or action) attitudes, sometimes also described as instrumental action attitudes, refer to behavioral algorithms and instructions that people follow in different social contexts. These attitudes are directly related to group norms and expectations set by significant social groups or reference groups. They translate the emotional and cognitive evaluations from relational and perceptual positions into concrete actions.
For example, the norms that regulate behavior in the workplace or within a family are based on conduct attitudes. These approaches are often less flexible than their relational and perceptual counterparts because they are tied to established rules and social conventions.
Consequently, while perceptual attitudes may evolve gradually with new experiences or learning, conduct attitudes tend to be more stable and relatively resistant to change unless significant change occurs in the basic social or emotional landscape.
Although classified separately, these attitudes are deeply interrelated. A person's emotional (relational) response to an event can trigger specific cognitive evaluations (perceptual attitudes), which are then translated into conduct attitudes (action). Feedback from the environment may strengthen or change each of these types of attitudes, emphasizing the dynamic interrelationships between them.
For example, a traumatic personal experience (experiential stimulus) may initially change perceptual evaluations; However, over time, the social attitudes picked up from influential reference groups may resist or moderate the initial change. This dynamic highlights the complexity of shaping and changing attitude, where social influences, personal experiences, and inherent biological factors all contribute to shaping our overall relationship to the world.
In conclusion, understanding the classification of attitudes into relational, perceptual and conduct types provides a comprehensive view of how people process information and interact with their environment. Each category plays a separate role – emotional, cognitive and behavioral – but together they create an integrated system that affects social perception, personal adaptation and group dynamics.
As mentioned, our theory behind the model of the "self" divides the human mental mechanism into two broad areas:
The primary self (predetermined biological core but capable of development): This includes, among other things, innate biological structures, instinctive emotional and cognitive processes, and seven channels of sensitivity (including the "threat channel"). These channels determine how a person reacts to stressors, where the threat channel is critical in assessing danger.
The secondary or social self:
It consists of internalized characters – organized into a hierarchical board or directorate of internalized characters (including a dominant "inner leader"), a group of internalized enemies, and a group of self-representations.
The "internalized characters’ board" group usually reflects internalized influential figures from the environment including virtual influential figures from literature and more and a representation of the subculture, while the "internalized enemies’" group contains negative representations of those who are perceived as threatening.
We suggest that using this framework, we can understand paranoid disorder as arising from an imbalance and dysfunction within internal structures:
A] Over-activation of the threat sensitivity channel:
The threat channel – one of the seven innate sensitivity channels – is responsible for detecting danger. In people with paranoid disorder, this channel may be oversensitive, causing even neutral or ambiguous social cues to be perceived as potential threats.
B] The dominance of the group of internalized enemies:
Under normal circumstances, the board of internalized characters (which includes, among other things, positive and balanced characters) helps to provide reactions to external events. In the paranoid person, however, the internalized enemy group becomes quite prominent.
This group represents the internalized negative and threatening characters, and is usually activated following traumatic or intense experiences. When these negative representations dominate, they tilt the person's internal dialogue towards suspicion and fear and it is possible that negative characters from it seep into the board of directors. Or the balance between her and the board of directors is violated in favor of a greater prominence of the enemy group within which certain figures or representatives of certain bodies become leaders and rise in the hierarchy.
However, it seems that in the case of de Clérambault's syndrome or erotomania, in which the paranoid patient believes that a famous personality is in love with him, there is a change in the board of directors and this figure becomes dominant and overshadows the previous internal leader.
C] The role of the internalized leader in the board of figures
The "inner leader" on the internalized characters’ board typically regulates which characters are admitted to the board. In paranoid disorder, it is also possible that this inner censor may be overly vigilant or biased, rejecting benign information and favoring interpretations consistent with a hostile worldview. The result is cognitive and emotional filtering in which neutral stimuli are represented as threatening.
D] Distorted relational, perceptual and conduct attitudes:
Relational attitudes: In terms of emotional evaluations of others, a dominant and internalized perspective of distrust is created, as the individual is on constant alert for betrayal or harm.
Perceptual attitudes: These are the cognitive frameworks that shape how a person interprets the world. An overemphasis on threat creates a worldview in which the actions of others are perceived as intentionally harmful.
Conduct Attitudes: As a result of biased relational and perceptual attitudes, the individual's behavior and actions may become defensive or aggressive in advance, further isolating them socially.
E] Synthesis
In summary, when we map the DSM-5R description of paranoid disorder to this model:
Biological predisposition: Innate sensitivity—particularly in the threat channel—may cause the individual to overreact to perceived dangers.
Victor Vicens et al. reported about the evidence of brain abnormality in the medial frontal/anterior cingulate cortex and insula in delusional disorder. ( Victor Vicens, Joaquim Radua, Raymond Salvador, Maria Anguera-Camós, Erick J. Canales-Rodríguez, Salvador Sarró, Teresa Maristany, Peter J. McKenna and Edith Pomarol-Clotet. Structural and functional brain changes in delusional disorder. The British Journal of Psychiatry , Volume 208 , Issue 2 , February 2016 , pp. 153 – 159 ).
By drawing on recent advances in the biological, computational and psychological processes of reinforcement learning, memory, and perception it may be feasible to account for delusions in terms of cognition and brain function. The account focuses on a particular parameter, prediction error – the mismatch between expectation and experience – that provides a computational mechanism common to cortical hierarchies, frontostriatal circuits and the amygdala as well as parietal cortices. (PR Corlett, ,JR Taylor , X-J Wang, PC Fletcher , JH Krystal . Toward a Neurobiology of Delusions. Prog Neurobiol. 2010 Jun 15;92(3):345–369.)
According to Linlin Fan et al., paranoia is associated with right amygdala hyperconnectivity with PFC, frontal cortex, and insula. (Linlin Fan, Hans Klein ,Emily Bass ,Cassi Springfield, Amy Pinkham. Amygdala hyperconnectivity in the paranoid state: A transdiagnostic study. Journal of Psychiatric Research Volume 138, June 2021, Pages 117-124).
Kapur proposed that a dysregulated, hyperdopaminergic state, at a “brain” level of description and analysis, leads to an aberrant assignment of salience to the elements of one’s experience, at a “mind” level. He saw delusions as a cognitive effort by the patient to make sense of these aberrantly salient experiences, whereas hallucinations reflect a direct experience of the aberrant salience of internal representations (Shitij Kapur, M.D., Ph.D., F.R.C.P.C. Psychosis as a State of Aberrant Salience: A Framework Linking Biology, Phenomenology, and Pharmacology in Schizophrenia. American Journal of Psychiatry Volume 160, Number 1).
Kaustubh Supekar et al. investigated the role of the celebral sorting.
In a normal case, the brain's cognitive filtering system – aka the salience network – works behind the scenes to selectively direct our attention to important internal thoughts and external events. With its help, we can dismiss irrational thoughts and unimportant events and focus on what's real and meaningful to us, such as paying attention to traffic so we avoid a collision.
Another brain circuir, the ventral striatum, a small brain region, and associated brain pathways driven by dopamine, play an important role in predicting what will be rewarding or important.
In their study the researchers found that the brain signatures of 22q11.2DS-associated psychosis overlap with those of idiopathic early psychosis in the salience network and dopaminergic reward pathway, providing substantial empirical support for the theoretical aberrant salience-based model of psychosis. (Supekar, K., de los Angeles, C., Ryali, S. et al. Robust and replicable functional brain signatures of 22q11.2 deletion syndrome and associated psychosis: a deep neural network-based multi-cohort study. Mol Psychiatry 29, 2951–2966 (2024).)
Kiyoshi Morimoto et al. argued that their molecular genetic analysis of delusional patients revealed the possible involvement of gene polymorphisms for DRD2 and DRD3 and its synthesizing enzyme (TH). (Kiyoshi Morimoto MD, Ph.D, Ryosuke Miyatake MD, Ph.D, Mitsuo Nakamura MD, Ph.D, Takemi Watanabe MD, Ph.D, Toru Hirao MD, Ph.D & Hiroshi Suwaki MD, Ph.D. Delusional Disorder: Molecular Genetic Evidence for Dopamine Psychosis. Neuropsychopharmacology 26, 794–801 (2002).
Internal dynamics: The early development of the self, which includes both a combination of positive internalized figures (from caregivers and significant others) and the formation of an internalized enemies’ group, can become unbalanced. In paranoid disorder, traumatic or significant experiences can tip the balance so that negative and threatening figures gain undue prominence.
A study conducted by Ayse Arikan suggests that people with a history of emotional abuse and higher attachment anxiety tend to have higher PPD symptoms. (Ayse Arikan. THE RELATIONSHIP BETWEEN CHILDHOOD TRAUMA AND PARANOID PERSONALITY DISORDER SYMPTOMS. https://academicworks.cuny.edu/cc_etds_theses/620/).
Internal censorship and misinterpretation: The role of the inner leader in filtering and integrating external stimuli becomes biased, leading to overactive internal censorship that emphasizes danger and distrust. This bias affects the person's relational, perceptual, and behavioral attitudes, creating a self that consistently anticipates harm from others.
Thus, according to DSM-5R and by this theoretical framework, paranoid disorder can be understood as a pathological condition in which a person's primary self (with its innate threat sensitivity) and secondary self (with its internalized figures and enemies) interact in a way that overwhelmingly favors a hostile interpretation of the world. This internal imbalance leads to the persistent suspiciousness and distrust of others that is central to the disorder.
In general, it seems that the interrelationship between the internalized characters’ board and the internalized enemies’ group is a dynamic and complex process that significantly affects the person's inner world – and consequently his behavior and perceptions in everyday life. Below is a breakdown of this relationship:
Internalized Characters’; Board:
Definition: This board consists of internalized representations of influential figures in a person's life – parents, teachers, mentors, and even admired fictional characters.
Function: These internalized figures serve as guides and regulators. They are organized hierarchically, with a dominant “inner leader” playing a key role in interpreting experiences and filtering incoming information. Their collective purpose is to help a person navigate social interactions, shape attitudes, and create expectations about relationships.
Definition: In contrast, the internalized enemies’ group consists of representations of figures who are perceived as threatening, hostile, or dangerous. These may stem from early negative experiences, traumatic events, or perceived betrayals.
Function: This group acts as a defensive buffer—a kind of psychological “blacklist” that marks potential dangers. It is designed to help a person stay alert to threats; however, when over-activated, it can lead to widespread distrust and misinterpretation of benign social cues.
Dynamic Interactions
Ongoing Dialogue and Competition:
The board of directors and the enemies’ group are in constant, usually unconscious, “interaction.” Under normal circumstances, the internal leader and the broader board moderate and balance the influence of the enemies’ group, ensuring that the threats are recognized but not exaggerated.
When faced with a situation, both groups evaluate it: the board may provide a relatively balanced and contextual interpretation, while the enemies’ group emphasizes potential risks or dangers. This internal discussion shapes how the individual perceives and responds to the world.
Influence on attitudes and perceptions:
Relational attitudes: The internalized characters’ board tends to foster more adaptive emotional responses—trust, empathy, and understanding—by recalling past supportive interactions. In contrast, when the enemies’ group has a stronger influence, relational attitudes may lean toward suspicion, fear, and hostility.
Perceptual attitudes: Cognitive interpretations of social situations are filtered through these internal representations. If enemies’ group perspectives dominate, neutral or ambiguous events can be perceived as malicious or threatening, reinforcing a worldview saturated with distrust.
Conduct attitudes: The resulting behavioral responses can range from cautious withdrawal to overt defensive or aggressive actions. Imbalance – when the enemies’ group overshadows the moderating influence of the board – can lead to overly defensive or aggressive actions as the individual attempts to ward off perceived threats.
Mechanisms of Regulation and Disregulation
Internal Censorship and Integration:
The “inner leader” within the board of characters acts as a gatekeeper, determining which representations are integrated into the board. Under healthy conditions, this helps to blend positive and negative internalization, ensuring that the person can distinguish between real danger and unfounded suspicion.
However, in cases of dysregulation – such as those seen in paranoid disorders – this internal censorship can be biased. It can give excessive weight to messages coming from the enemies’ group, and in effect “inject” too many negative and threatening representations.
Responsiveness to external stimuli:
The dynamic interplay becomes particularly pronounced when a person is experiencing stress or trauma. External cues may activate the enemies’ group, triggering a chain of defensive responses. Even if the character board attempts to offer a balanced interpretation, the heightened state of alertness may cause the enemies’ group to dominate the internal dialogue.
Over time, this imbalance can lead to a self-reinforcing cycle: as enemy representations become stronger, the inner leader may adopt a defensive stance, further entrenching paranoid perceptions and behaviors.
Clinical Implications
In a clinical context – particularly within the DSM-5R conceptualization of paranoid disorders – this imbalance is critical:
Excessive Suspicion: An overly active internalized enemies’ group, uncontrolled by the moderating board, causes persistent and pervasive suspicion of the motives of others.
Misinterpretation of Social Cues: The threat bias leads to misinterpretation of benign or ambiguous actions as hostile, contributing to difficulties in relationships and social functioning.
Defensive Behaviors: The individual may exhibit overly cautious behaviors or even aggressive defensiveness, as a means of self-protection from perceived dangers.
In essence, the healthy functioning of a person's inner world relies on a delicate balance: the board of internalized figures must regulate and integrate experiences in a way that fosters adaptive social behaviors, while the internal enemy group must remain a background warning system rather than a dominant force.
When the enemies’ group becomes overly influential – whether through traumatic events or through faulty internal censorship – the resulting internal dialogue may bias the individual's relational, perceptual, and behavioral attitudes toward a paranoid worldview.
These dynamic interactions help explain many of the core characteristics of paranoid disorders, as defined in the DSM-5R, where the individual's internal conflict leads to widespread distrust, misinterpretation of social cues, and defensive behaviors.
We will add that the internalized enemies’ group is a special repository within the self that collects and stores negative images and representations related to threats. These are symbolic and emotionally charged images derived from past traumatic experiences, negative interactions, or perceived threats.
Here we will detail what happens specifically in this group:
Formation and Storage
Early in life, when a person experiences situations of fear, betrayal, or trauma, parts of these experiences are encoded as negative representations. These representations are segregated into the internalized enemies’ group as a defense mechanism.
Emotional labeling:
Each representation stored in this group is accompanied by strong negative emotions – fear, anger, or distrust – that serve as a warning signal for future encounters. These emotional labels ensure that any similar cues later on are quickly recognized as dangerous.
Activation and dynamics
When an external stimulus or interpersonal situation contains elements reminiscent of past threats, the internalized enemies’ group is activated. This rapid response system is designed to alert the individual to potential danger even if the threat is vague or mild.
Perceptual bias:
Once activated, the enemies’ group influences the individual's perceptual and cognitive processes. Neutral or even positive stimuli may be misinterpreted as threatening because the internal enemy representations cast a shadow over incoming information. This leads to a distorted worldview, in which distrust and suspicion prevail.
Conflict with other internal structures:
In healthy circumstances, the dominant figures in the inner board help to moderate and contextualize the input of the enemies’ group. However, if the enemy group becomes too dominant—often due to repeated or intense traumatic experiences—the balance is disrupted. The inner board leader may begin to over-prioritize these negative representations, further reinforcing defensive and paranoid attitudes.
Behavioral and Experiential Implications
Defensive Responses:
Activation of the internalized enemies’ group often results in defensive behaviors. The individual may become overly cautious, preemptively aggressive, or socially withdrawn as a way to protect themselves from the perceived, omnipresent threat.
Persistent Suspicion:
Over time, repeated activation reinforces a persistent sense of distrust of others. The individual may be unable to fully integrate positive social experiences, as the enemy group continually reinforces a narrative of danger and betrayal.
Because the enemies’ group represents a part of the self that is in constant conflict with more balanced and adaptive internalizations (those held in the inner board), there can be a continuous internal struggle. This conflict contributes to the instability of self-representation and exacerbates symptoms of paranoia. However, the infiltration of enemies’ group figures into the board cannot be ruled out.
Regulatory challenges
Representations within the enemies’ group are often rigid and resistant to change because they were formed under conditions of high emotional arousal. This rigidity makes it difficult for the individual to reappraise past events or change their perception of threat, even when evidence suggests that the danger no longer exists.
Impact on relationships:
Because the enemies’ group biases the interpretation of interpersonal cues, this can lead to chronic misunderstandings and conflict in relationships.
The individual may perceive good behaviors as hostile, creating a self-fulfilling prophecy of isolation and further strengthening of the enemies’ group's influence.
In summary, the internalized enemy group functions as an alarm system, which, while initially protective, may become overactive and dysregulated. It stores and perpetuates negative representations that bias perception, distort social interactions, and contribute to a cycle of distrust and defensive behavior, all of which are central to the expression of paranoid disorders.
The internalized enemies’ group can expand and increasingly influence the overall structure of internalized figures, including representations of the "self." This process can develop as follows:
Cumulative effect of traumatic experiences:
Repeated exposure to trauma or ongoing interpersonal stress may lead to the formation of more negative representations. Each new experience interpreted as threatening may contribute additional figures to the enemy group and cause it to expand over time.
Reinforcement through hypervigilance:
When the threat channel is chronically activated, the individual's internal system becomes primed to detect danger. This can lead to overgeneralization, in which even mild or vague situations are interpreted as threats. The constant activation reinforces existing enemy representations and may lead to the formation of new ones.
Under normal circumstances, the internalized character palette (which includes positive, balanced representations) restrains the enemies’ group. However, as the enemies’ group expands, it can begin to upset this balance. The internal leader—the gatekeeper who regulates which representations are allowed into the conscious self—may begin to prioritize input from the enemies’ group if it perceives this threat as paramount.
As the enemies’ group grows, it can overshadow the more adaptive and supportive figures in the internalized board. The result is a biased internal dialogue, in which negative interpretations become the default mode. In extreme cases, the enemies’ group can take over the internalized board, leading to a pervasive state of distrust and suspicion.
Impact on “Me” Representations
Self-representations are evolving self-images that incorporate experiences, attitudes, and internalized characters. As the enemies’ group becomes more salient, these self-representations begin to include elements of hostility, defensiveness, and fear. This means that the individual's self-concept becomes more aligned with a worldview in which threat and betrayal are expected.
Internal conflict and identity distortion:
As the enemies’ group takes on a larger role, the balanced aspects of self-representations that may include compassion, trust, and openness can diminish. This internal conflict—between a protective but increasingly paranoid enemies’ group and a moderating board—can result in a fragmented or distorted sense of identity. The individual may see themselves as perpetually under siege or inherently vulnerable, further reinforcing the paranoid attitude.
In conclusion, the internalized enemies’ group can indeed expand under conditions of repeated or intense threat. As it grows, it may gradually take over the regulatory functions of the internalized figures’ board. This shift in balance also significantly affects the "self" representations, which feed on the board group and instill a persistent sense of distrust and defensiveness in the individual's self-concept.
The result is a self-system that is heavily biased towards a dangerous worldview, the hallmark of paranoid disorder as conceptualized in the DSM5R framework.
Incidentally, similar ideas have been proposed in the past, particularly within the psychoanalytic and object relations frameworks. Over the years, theorists have explored how early relational experiences lead to the internalization of both positive and negative aspects of significant others. Here are some historical perspectives:
The following is a summary of the psychoanalytic literature that specifically addresses paranoia – in its pathological forms such as paranoid disorder, paranoid psychosis, or what is sometimes called "paranoia vera":
Melanie Klein's Contribution to Paranoid Anxiety
Klein's conception of the paranoid-schizoid position describes how an early splitting of the self and its objects produces intense persecution anxieties.
In cases where integration fails, these early defenses can develop into chronic distrust and obsessions—core features of paranoid disorder or paranoid psychosis (often called "paranoia vera").
Fairbairn's insights into internalized obsessional objects
In 1952, Fairbairn emphasized that the internalization of hostile and punitive representations can lead to a dominant internal "enemy" that shapes the individual's perception of others as inherently dangerous. When these internalized persecutory figures become dominant, the resulting internal environment can cause the individual to develop paranoid ideation or full-blown paranoid psychosis.
Kernberg's Model of Paranoid Pathology
Kernberg's work on personality organization expands on these ideas by linking the dominance of primitive defenses—especially splitting—to a fragmented inner world. In cases where splitting is extreme and internalized negative (persecutory) elements predominate, the individual may exhibit symptoms of paranoid personality disorder or paranoid psychosis.
This framework helps explain how "paranoia vera" arises from a failure to integrate conflicting internal representations, resulting in a pervasive sense of distrust and threat.
Empirical and Clinical Perspectives on Paranoid Ideation
A study combining object relations assessments has found that a lack of integration between positive internalized and persecutory representations is strongly associated with paranoid ideation. Studies using measures such as the Social Cognition Scale and the Object Relations Scale suggest that when persecutory representations predominate, patients are more likely to develop persistent paranoid symptoms, consistent with the clinical picture of paranoid psychosis or paranoid disorder.
In conclusion, the psychoanalytic theories of Klein, Fairbairn, and Kernberg provide a coherent framework for understanding how early paranoid anxieties and the internalization of hostile and persecutory figures can lead to the development of paranoid disorder, paranoid psychosis, or "paranoia vera."
These ideas emphasize that when the internal enemies’ group dominates the inner world—due to failures to integrate fragmented aspects of the self—chronic distrust and persecutory ideas may arise, which characterize the pathology seen in these conditions.
References to psychoanalytic approaches
Klein, M. (1946). Notes on some schizoid mechanisms. In The Selected Melanie Klein (pp. 157–181). Hogarth Press.
Fairbairn, W. R. D. (1952). Psychoanalytic Studies of the Personality. Tavistock Publications.
Kernberg, O. F. (1975). Borderline Conditions and Pathological Narcissism. Jason Aronson.
Kernberg, O. F. (2014). The Treatment of Patients with Borderline Personality Organization: Contemporary Developments. Routledge.
Porcerelli, J. H., & Blatt, S. J. (2011). Object relations and defense mechanisms in personality disorders: Internal representations and their clinical implications. In S. K. Huprich (Ed.), Advances in the Assessment of Object Relations in the 1990s (pp. 317–343). Lawrence Erlbaum Associates.
However, we note that the article does take an integrative approach by combining the clinical and diagnostic framework of DSM-5-TR with psychoanalytic theories and self-model-based approaches. It attempts to bridge theories that focus on symptoms and diagnostic criteria with approaches that emphasize internal dynamics, personal development, and the relationships between internal representations (such as the board group and the internalized enemies’ group).
Finally, we note that the above article has a number of weaknesses that include potential tensions or contradictions:
Separation versus integration of approaches:
On the one hand, the DSM approach focuses on clear diagnostic definitions (e.g., the absence of other psychotic symptoms), and on the other hand, the integrative model attempts to explain the disorder as a result of a dynamic imbalance between internal components – which may be perceived as a blindness to the separation between symptoms and internal mechanisms.
Thus, there is a conflict between the categorical approach of the DSM and the dynamic and personal explanation presented in the self model.
Biological versus psychological assumptions:
The article presents both biological factors (such as innate sensitivity to the threat channel) and psychological-developmental factors (such as the internalization of significant figures and the creation of an internalized enemies’ group). This leads to tension as different approaches may emphasize different factors as primary drivers – which can sometimes create conflict in theory if a unified explanation is required.
Addressing normal appearance outside of the psychotic context: According to the DSM-5-TR, people with paranoid disorder typically function normally outside of the context of delusions.
In contrast, the integrative model describes a dynamic internal system in which each part (such as the internalized enemy group or the board of directors) influences worldview and emotional response in an ongoing manner—which may raise the question of how “normal” functioning can be combined with a transparent and fixed internal system that leads to hostile interpretations.
In conclusion, although the article aims to integrate and expand the understanding of paranoid disorder, it can be seen as a theoretical tension between the approaches – mainly between the symptomatic clinical explanation of the DSM and the deep-psychodynamic explanation that attempts to integrate biological, personality, and developmental factors.
These tensions are not necessarily an "error" but rather reflect the difficulty of integrating different theoretical approaches into a single unified framework, and constitute a challenge in the research and understanding of complex mental disorders.
That's it for now,
Dr. Igor Salganik and Prof. Joseph Levine
Leave a comment